


Editorial & Legal Accuracy Notice (Louisiana)
This blog contains general legal and safety information and is not legal advice. Laws and deadlines can change, and outcomes depend on specific facts.
Last reviewed / updated: March, 2026
Reviewed, updated, and authored by: Stephen Babcock, Louisiana injury lawyer
This guide explains typical herniated disc recovery phases, red flags, and a documentation plan that protects both your health and a Louisiana injury claim.
A MedlinePlus herniated disk overview explains that disc material can press on or irritate nerves, which is why pain may travel into an arm or leg. In plain terms, herniated disc recovery is often about calming the irritated nerve and rebuilding daily tolerance. This page walks through common timelines, testing choices, and proof gaps that matter when an insurer gets involved. Because a CDC data brief on back pain shows back pain is common, insurers often look for “pre-existing” explanations, so clean documentation matters.
If you are inside the first 72 hours, call (225) 500-5000 or use the free case review form before evidence changes.
Firm links: Client Reviews | Contact | Locations
Download the printable toolkit (PDF) if you want the recovery phases, red flags, and proof checklist in one handout. It is designed to be easy to print and easy to share with a family member helping you keep records.
How Long Does Herniated Disc Recovery Take?
A Cleveland Clinic herniated disk overview notes that many people improve within about four to six weeks with conservative care. Mayo Clinic guidance on herniated discs explains that recovery varies based on nerve irritation, weakness, and how well symptoms trend over time, so look for steadier function and fewer flare-ups rather than a single “magic day.”
- First 72 hours: get evaluated, capture onset details, and start a simple symptom-and-function log.
- Weeks 1–2: focus on safe movement and consistent care so the record matches what you feel.
- Weeks 3–6: rebuild tolerance with PT or home exercises and track progress in real-world tasks.
- Beyond 6 weeks: persistent weakness, severe symptoms, or repeat flares often change the care plan.
First 72 Hours: The Evidence Clock
In the first three days, you are usually answering two questions at once: what is happening medically and what changed after the event. If the disc injury followed a wreck, the early facts often overlap with your injury claim, so keep records aligned with the same timeline you would use for a Baton Rouge car accident case.
- Write down when pain started, where it travels, and what movements trigger it.
- Save visit summaries, prescriptions, and any work restriction notes.
- Photograph visible injuries and preserve relevant property or vehicle photos.
- Do not “tough it out” in silence if numbness or weakness is worsening.
This is why we push evidence preservation early: once a record goes missing, insurers often fill the gap with their own explanation. That is what we mean by leverage when we say timelines beat opinions.
Weeks 1–2: Calm the Irritated Nerve
During early herniated disc recovery, symptoms can bounce around, especially if a nerve is irritated. A Johns Hopkins overview of lumbar disc disease notes that symptoms depend on which disc and nerve are involved, so your limits may look different than someone else’s.
- Track function: sitting tolerance, standing tolerance, walking distance, and sleep quality.
- Write down “what changed” after each visit or PT session in one sentence.
- Keep missed-appointment reasons documented if life gets in the way.
Weeks 3–6: Rebuild Tolerance
Weeks three through six often look like gradual exposure to normal tasks, with fewer sharp flares and more predictable limits. The key is not perfection; it is consistent documentation that shows the trend line in herniated disc recovery.
- Keep PT notes, home exercise plans, and work notes together in one folder.
- Record flare triggers like long drives, lifting, or prolonged sitting.
- Update your log when a new symptom appears, not a week later.
After 6 Weeks: When Care Often Changes
If you still have significant leg pain, weakness, or repeated setbacks, your clinician may discuss imaging, injections, or a specialist referral. An AAOS OrthoInfo explainer on lumbar herniated discs describes conservative care as the usual starting point while also noting that certain persistent or severe symptoms can change treatment decisions.
- Ask your provider to document why the plan is changing and what finding prompted it.
- Keep updated work restrictions current, not implied.
- Preserve a clean list of medications and side effects if they affect function.
What Symptoms and Red Flags Matter During Herniated Disc Recovery?
Mayo Clinic’s herniated disk overview explains that a herniated disc can cause back or neck pain plus numbness, tingling, or weakness when a nerve is affected. Cleveland Clinic’s cauda equina syndrome guide lists bladder or bowel changes and worsening leg weakness as emergency warning signs that need urgent evaluation.
- Emergency red flags: new bladder or bowel problems, groin or saddle numbness, rapidly worsening weakness.
- Nerve-pattern symptoms: pain that shoots down an arm or leg, tingling, numbness, or focal weakness.
- Function signals: stumbling, foot drop, unsafe lifting limits, or sleep disruption that does not improve.
- Insurance-proof signals: treatment gaps, inconsistent symptom descriptions, or missing work notes.
Not every scan finding equals pain, and not every pain pattern shows up cleanly on imaging. A Mayo Clinic explanation of bulging discs notes that some disc changes can exist without symptoms, which is why the “before vs. after” story matters in both medical care and claims.
If you notice new weakness, worsening numbness, or bowel or bladder changes, treat it as a medical urgency first and a legal issue second. Your health comes first, and the record that follows is often the record the insurer reads later.
When Do You Need Imaging or Other Tests for a Herniated Disc?
Mayo Clinic’s diagnosis and treatment guidance explains that clinicians combine history, physical exam, and testing when needed to evaluate a suspected herniated disc. An AAOS OrthoInfo article on lumbar disc herniation describes imaging as one tool among several, often used when symptoms persist or neurological concerns show up on exam.
| Test | What It Can Help With | Why It Matters for Documentation |
|---|---|---|
| MRI | Shows soft tissue, discs, and nerve compression patterns. | Pairs best with a dated symptom timeline and neuro exam findings. |
| X-ray | Looks at bone alignment and fractures, not discs directly. | Helps rule out some issues while the disc diagnosis remains clinical. |
| CT | More detail than X-ray for bone, sometimes used when MRI is not an option. | Useful when the chart explains why MRI was delayed or unavailable. |
| EMG/NCS | Evaluates nerve function when symptoms and imaging do not line up. | Can document objective nerve irritation when the defense says “no proof.” |
In herniated disc recovery, the most common proof gap is not “no MRI,” it is “no explanation.” If your clinician delays imaging, ask them to document the medical reason, because that single line often prevents the insurer from framing it as “not serious.”
If your disc injury is part of a broader musculoskeletal picture, you may also find our Baton Rouge orthopedic injuries page helpful as an overview of how orthopedic documentation tends to work in injury cases.
What Treatment Options Shape Herniated Disc Recovery?
An AHRQ topic overview on herniated disk treatment describes common paths that start with conservative care and escalate only when symptoms persist or worsen. Mayo Clinic’s treatment guidance describes options like medications, physical therapy, injections, and surgery depending on symptoms and exam findings.
- Activity changes: adjust movements to reduce nerve irritation while staying safely mobile.
- Physical therapy: build strength and tolerance with a clear plan and dated progress notes.
- Medication plan: use clinician-guided meds and document side effects that affect function.
- Injections: sometimes used to reduce inflammation and help you participate in rehab.
- Surgical discussion: more common when weakness or severe symptoms persist despite care.
If surgery becomes part of the conversation, keep the “why now” clearly documented. The insurer will often focus on whether the disc problem was present before the event, so the decision-making notes matter as much as the procedure description.
That is what we mean by leverage on the medical side: the chart should explain the reasoning in plain language, not just list services. When the record tells the story, insurers have less room to rewrite it.
How Do You Build a Timeline for Herniated Disc Recovery?
A good timeline makes medical care more consistent and makes claim questions easier to answer. In herniated disc recovery, the goal is a simple sequence that connects dates, symptoms, and function without exaggeration.
- Event date: what happened and what you felt first, including radiating pain or numbness.
- First medical contact: where you went and what was documented on exam.
- Daily function notes: sitting, walking, sleep, driving, lifting, and missed work.
- Treatment steps: PT start date, home exercises, medication changes, injections, referrals.
- Testing milestones: imaging dates and the clinician’s reasoning for ordering or delaying tests.
- Turning points: “better,” “worse,” or “new symptom” events with a date and trigger.
This is why we build the timeline before anyone asks for a recorded statement: it prevents rushed answers and accidental inconsistencies. A timeline also helps your provider document work restrictions that match your actual limits.
| What to Track | Write It Down Like This |
|---|---|
| Pain location | “Left low back into calf” beats “my back hurts everywhere.” |
| Function limits | “Can sit 15 minutes” beats “can’t sit long.” |
| Care consistency | “Missed PT due to flu, rescheduled” beats silence. |
| Work restrictions | “No lifting over 10 lbs for 2 weeks” beats “light duty.” |
What Do Insurers Question in Herniated Disc Claims?
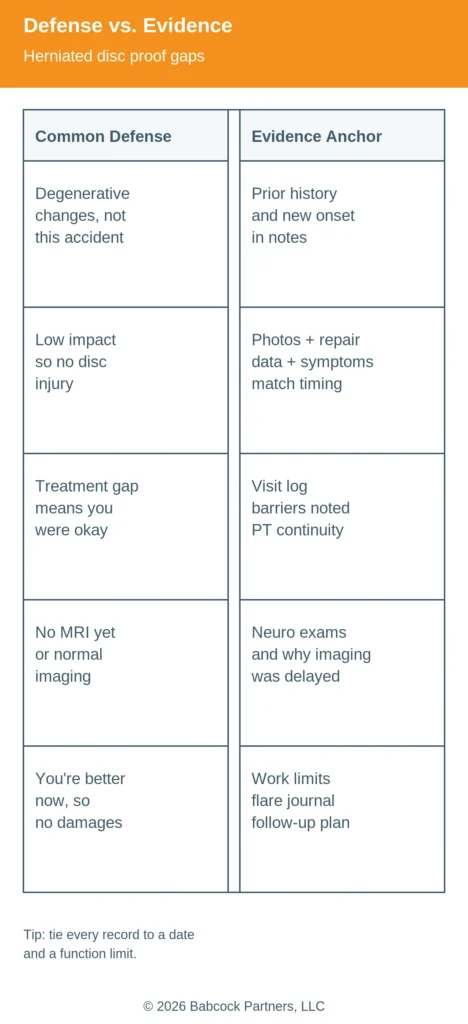
Insurance adjusters often do not argue about pain; they argue about causation, consistency, and gaps. In a herniated disc recovery case, the most common defense themes are “degeneration,” “low impact,” “gap in treatment,” and “you are fine now.”
| Common Defense Angle | Evidence Anchor That Helps |
|---|---|
| “This is degenerative, not from the event.” | Prior history review plus dated onset notes and a clear “before vs. after” change. |
| “The crash or incident was minor.” | Photos, repair records, witness notes, and function limits that match symptom timing. |
| “You waited too long to treat.” | Visit log, barriers documented in writing, and consistent symptom reporting across visits. |
| “No MRI” or “imaging doesn’t prove it.” | Neuro exams, PT findings, and documented reasons for testing decisions. |
| “You improved, so the claim is over.” | Work restrictions, flare journal, follow-up plan, and lingering limits on daily activities. |
That is what we mean by leverage against insurer tactics: you do not “win” by arguing louder, you win by closing proof gaps early. If an adjuster pushes for a broad release or a quick settlement while your symptoms are still changing, treat it as a signal to slow down and document, not a signal to rush.
How Does a Herniated Disc Fit Into a Louisiana Injury Claim?
Under La. Civ. Code art. 2315, a person who causes injury through fault can owe damages. La. Civ. Code art. 2316 explains that negligence can create that responsibility, which is why documentation and causation questions matter.
- Fault: who caused the event and what evidence supports it.
- Medical causation: what changed after the event and how providers recorded it.
- Damages: how symptoms affected daily life, work, and the need for care.
- Comparative fault issues: what the insurer claims you did wrong and how the record answers it.
Herniated disc claims commonly follow collisions, workplace incidents, and serious falls, but the proof strategy is often similar. If your injury happened on the job, our Baton Rouge workplace injury attorney page explains how evidence and employer reporting issues can shape the early record.
If workers’ comp is involved, you may also need to coordinate treatment and paperwork with a comp claim, which can create gaps if not handled carefully. Our Baton Rouge workers’ compensation page covers common friction points so you can keep your medical timeline consistent.
What we see in practice
We see disc injuries get minimized when early records are thin, symptoms are described differently at each visit, or work restrictions are missing. We also see insurers lean hard on “degeneration” when the timeline is unclear, even when the person had no meaningful limits before the event.
- Gaps create narratives: if care pauses, insurers often claim symptoms resolved.
- Function beats adjectives: “can’t sit 20 minutes” is stronger than “severe pain.”
- Imaging is not the whole case: the neuro exam and PT notes often carry the story.
- Early pressure is common: recorded statements and releases show up before treatment stabilizes.
What Should You Do During Herniated Disc Recovery to Protect Your Claim?
The goal is not to “build a case” by dramatizing symptoms; it is to keep the medical and real-life record accurate and consistent. During herniated disc recovery, small habits like a weekly log and organized paperwork reduce proof gaps that insurers target.
- Keep a dated symptom-and-function log that fits on one phone note page.
- Attend recommended follow-ups, and document barriers if you cannot.
- Ask providers to write clear work and safety restrictions, not vague “light duty.”
- Save photos, prescriptions, PT notes, and imaging reports in one folder.
- Be cautious with broad releases or quick settlements while symptoms are still changing.
Download the printable toolkit (PDF) if you want a simple template for the timeline and defense-audit checklist. It is meant to reduce stress and keep your records consistent, not to replace medical advice.
Louisiana Law Snapshot (Updated 2026)
La. Civ. Code art. 3493.1 sets a two-year delictual prescription period for many personal injury claims, which makes early evidence preservation and deadline spotting critical. As amended effective January 1, 2026, La. Civ. Code art. 2323 applies comparative fault and includes a 51% bar, meaning a claimant more than 50% at fault may not recover damages.
| Rule | What It Means | Practical Takeaway |
|---|---|---|
| Two-year prescription | The deadline to file can arrive faster than people expect. | Talk to a lawyer quickly if liability is disputed or records are incomplete. |
| Comparative fault + 51% bar | Fault is allocated by percentage, and being more than 50% at fault can block recovery. | Preserve objective evidence early so fault arguments do not harden. |
These rules are general, and the details can change based on facts, defendants, and timing. If you are near a deadline, or fault is being pushed onto you, it is safer to get legal advice early than to “wait and see.”
Free Case Review for Herniated Disc Injuries in Louisiana
If your symptoms are changing, your records need to keep up so the insurer cannot rewrite the timeline. Our Babcock Benefit approach focuses on fast evidence preservation and trial-ready preparation, without hype and without shortcuts.
We are not built for volume. We are built for leverage.
Call (225) 500-5000 and use the free case review form if you have worsening weakness, pressure to sign paperwork, or a growing gap between what you feel and what the chart says. The sooner we can map the first 72 hours, the easier it is to preserve proof before it disappears. Evidence fades quickly, and deadlines do not pause for “recovery time.”
These items are helpful to have with you when you call, but do not delay calling because you do not have them. If you have them handy, keep them nearby for the call.
- Crash report or incident report number and the date of the event
- Your first-visit paperwork and any imaging orders or results
- A short list of symptoms with dates and function limits
- PT or specialist appointment dates and any missed-visit reasons
- Work restriction notes and missed-time documentation
Call Today If
- You have new bladder or bowel changes, groin numbness, or worsening weakness
- An insurer is pushing for a recorded statement or a broad release
- You were told the injury is “degenerative” and your timeline is getting questioned
- Your work restrictions are missing, unclear, or not matching real limits
What Happens Next
- Evidence triage: we map the first 72 hours and identify missing records and proof gaps
- Deadline spotting: we flag Louisiana prescription issues and time-sensitive notice problems
- Insurer contact strategy: we help control what is said, when, and how it is documented